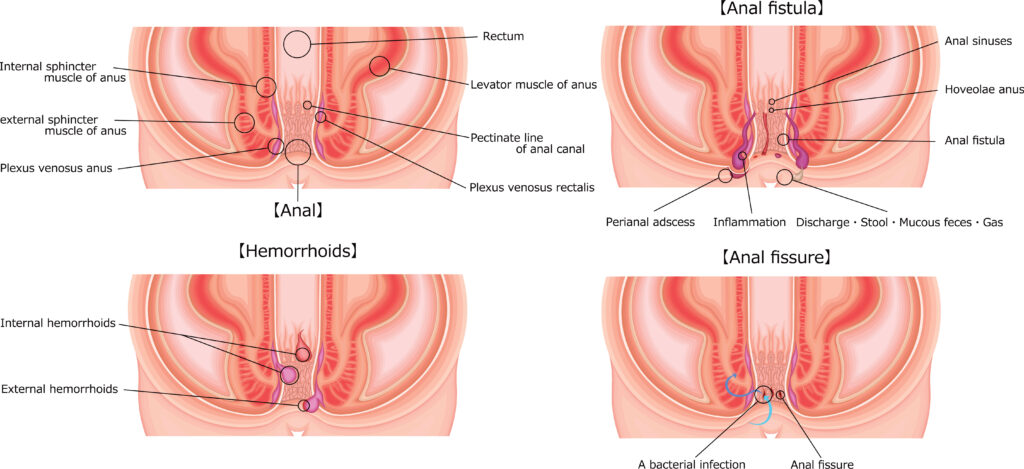
Anal fistula surgery is performed to treat an abnormal connection between the epithelialized surface of the anal canal and the perianal skin. Anal fistulas are often the result of an infection in an anal gland that leads to an abscess. Once the abscess is drained, a fistula can form. Surgical treatment is aimed at eradicating the fistula, promoting healing, and minimizing the risk of recurrence and complications such as incontinence.
Indications
Surgery is indicated for:
Persistent anal fistulas that do not heal with conservative treatment.
Recurrent infections or abscess formation.
Significant discomfort or drainage.
Types of Anal Fistula Surgery
Fistulotomy
Procedure: The fistula tract is opened and laid flat, allowing it to heal from the inside out.
Indications: Suitable for simple, superficial fistulas.
Advantages: High success rate with complete healing.
Disadvantages: Risk of incontinence, particularly with fistulas that pass through a significant portion of the sphincter muscle.
Seton Placement
Procedure: A seton (a piece of surgical thread) is placed through the fistula tract. It may be left loose to promote drainage and fibrosis or tightened gradually to cut through the fistula over time.
Indications: Complex or high fistulas involving a significant amount of sphincter muscle.
Advantages: Preserves sphincter function, reducing the risk of incontinence.
Disadvantages: Prolonged treatment duration with potential discomfort.
Advancement Flap Procedure
Procedure: The internal opening of the fistula is closed with a flap of healthy tissue.
Indications: Complex or recurrent fistulas.
Advantages: Lower recurrence rates with preserved sphincter function.
Disadvantages: More complex surgery with a longer recovery period.
LIFT Procedure (Ligation of the Intersphincteric Fistula Tract)
Procedure: The fistula tract is accessed and ligated in the intersphincteric space, then divided.
Indications: Suitable for intersphincteric and transsphincteric fistulas.
Disadvantages: Requires surgical expertise and has a variable success rate.
Fibrin Glue or Plug
Procedure: The fistula tract is filled with fibrin glue or a bioprosthetic plug to close it and promote healing.
Indications: Suitable for patients who prefer a less invasive option or have a high risk of incontinence.
Advantages: Minimally invasive with quick recovery.
Disadvantages: Lower success rate compared to other surgical options.
Procedure Steps for Fistulotomy
Preoperative Preparation
Medical evaluation and history.
Imaging studies (such as MRI or endoanal ultrasound) to map the fistula tract.
Instructions on fasting and bowel preparation if necessary.
Anesthesia
Local anesthesia with sedation, regional anesthesia, or general anesthesia, depending on patient preference and the extent of the surgery.
Surgical Procedure
Positioning: Patient is positioned in the lithotomy or prone position.
Incision: The surgeon makes an incision along the fistula tract.
Fistulotomy: The tract is opened and laid flat, removing any infected tissue.
Closure: The wound is left open to heal by secondary intention or closed with sutures, depending on the depth and location.
Postoperative Care
Pain Management: Pain relief medications as prescribed.
Wound Care: Keeping the surgical area clean and dry. Warm sitz baths can help reduce pain and promote healing.
Dietary Changes: High-fiber diet and adequate fluid intake to prevent constipation and straining.
Activity Restrictions: Avoid heavy lifting and strenuous activities for a few weeks.
Follow-Up: Regular follow-up visits to monitor healing and address any complications.
Risks and Complications
Infection: Risk of infection at the surgical site.
Bleeding: Some bleeding is normal, but significant or persistent bleeding should be reported.
Incontinence: Risk of temporary or permanent incontinence, particularly with procedures involving the sphincter muscles.
Recurrence: Although surgery aims to eradicate the fistula, there is a risk of recurrence.
Conclusion
Anal fistula surgery aims to remove the fistula tract, promote healing, and prevent recurrence while minimizing complications such as incontinence. The choice of surgical technique depends on the complexity of the fistula and the patient’s overall health. Proper preoperative planning, skilled surgical technique, and diligent postoperative care are essential for achieving the best outcomes and improving the patient’s quality of life. Regular follow-up and adherence to postoperative care instructions are crucial for a successful recovery.