Myringotomy is a surgical procedure involving a small incision in the eardrum (tympanic membrane) to relieve pressure caused by excessive fluid buildup or to drain pus from the middle ear. This procedure is often performed with the insertion of a tympanostomy tube to maintain drainage and prevent recurrent fluid accumulation.
Indications
Myringotomy is indicated for:
Recurrent acute otitis media (ear infections).
Chronic otitis media with effusion (persistent fluid in the middle ear).
Hearing loss due to middle ear fluid.
Barotrauma (ear pressure problems due to altitude changes).
Prevention of ear infections in children with frequent episodes.
Procedure Steps for Myringotomy
Preoperative Preparation
Evaluation: Comprehensive medical evaluation, including hearing tests and examination of the eardrum.
Anesthesia Discussion: General anesthesia is commonly used for children, while local anesthesia can be used for adults.
Instructions: Fasting before the procedure and any necessary medication adjustments.
Anesthesia
General Anesthesia: Typically used for children to ensure they remain still and comfortable.
Local Anesthesia: Can be used for adults, allowing the procedure to be done in an office setting.
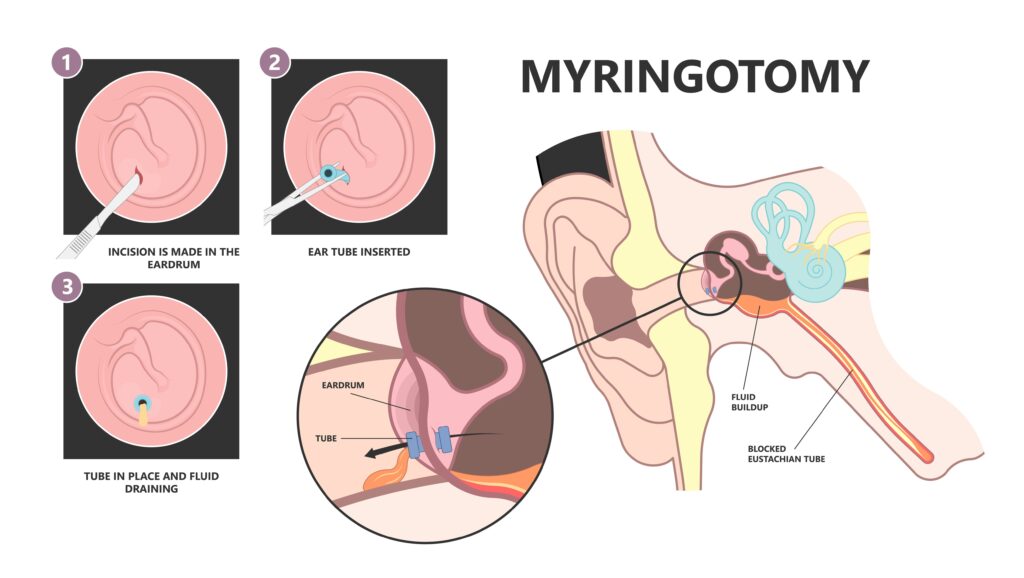
Surgical Procedure
Positioning: The patient is positioned with the affected ear accessible.
Incision: A small incision (myringotomy) is made in the eardrum using a scalpel or laser.
Fluid Removal: Fluid or pus is suctioned out from the middle ear.
Tube Insertion: A small tube (tympanostomy tube) may be inserted into the incision to maintain drainage and ventilation.
Postoperative Care
Pain Management: Pain is usually minimal, but analgesics can be prescribed if needed.
Ear Protection: Keeping the ear dry and avoiding water exposure (use of earplugs during bathing or swimming).
Activity Restrictions: Minimal restrictions; children can usually return to normal activities quickly.
Follow-Up: Regular follow-up visits to monitor the tube and ear health. The tube typically falls out on its own within 6-12 months.
Types of Tympanostomy Tubes
Short-term Tubes: Designed to stay in place for 6-12 months and then fall out naturally.
Long-term Tubes: Larger flanges designed to stay in place for a longer duration, may require removal by a physician.
Risks and Complications
Infection: Risk of postoperative ear infections.
Persistent Drainage: Continued drainage from the ear after the procedure.
Tube Blockage: The tube can become blocked with earwax or other debris.
Scarring: Minor scarring of the eardrum.
Hearing Changes: Temporary changes in hearing, usually improving as the ear heals.
Persistent Perforation: Rarely, the eardrum may not heal properly after the tube falls out, requiring additional surgical repair.
Recovery
Initial Recovery: Patients typically recover quickly with minimal discomfort. Children can often return to school the next day.
Long-Term Recovery: Regular monitoring to ensure the tube remains in place and the ear remains free of infection or fluid buildup. Most tubes fall out on their own within a year.
Conclusion
Myringotomy with or without tympanostomy tube insertion is a common and effective procedure to treat chronic ear infections, persistent middle ear fluid, and associated hearing loss. Proper preoperative evaluation, skilled surgical technique, and diligent postoperative care are essential for achieving the best outcomes. Regular follow-up is important to monitor ear health and manage any complications promptly. This procedure can significantly improve quality of life, especially for children with recurrent ear infections or hearing issues.